- Medial Rectus And Inferior Oblique Dmg Muscle
- Medial Rectus And Lateral Rectus
- Medial Rectus And Inferior Oblique Dmg Pain
- Medial Rectus Definition
- Medial Rectus And Inferior Oblique Dmg Muscles
- Medial Rectus Muscle Function
The superior rectus and inferior oblique muscles working together pull the eye upward without rotating the eye. To depress the eye while looking straight ahead, the inferior rectus and superior oblique contract together as the superior rectus and inferior oblique relax. The medial rectus, inferior rectus and inferior oblique nuclei connect to the ipsilateral muscle. The motor nuclei are distributed along the nucleus with three subgroups for the medial rectus. The levator palpebrae nuclei supplies both ipsilateral and contralateral function from a midline subnucleus.
Motor system 20. LR is the Lateral Rectus. MR is the Medial Rectus. SR is the Superior Rectus. IR is the Inferior Rectus. SO is the Superior Oblique. IO is the Inferior Oblique. 2: 2D-OPMM: front view. Left downward saccadic eye movement driven by medial rectus and inferior rectus as agonists, and lateral rectus and superior rectus as.
NBME 21 Answers ↦A 28-year-old man is brought to the emergency ..
Inferior rectus and inferior oblique🔍
submitted by dr_jan_itor(55), 2019-08-02T19:26:29Z
Option A is the only option where both muscles are part of the orbital floor.Also, the last sentence in the question stem is a total modifyer of what one would expect the question to be asking. It is not asking for you to assume that these muscles have been severed, paralyzed, or rendered flacid. It is asking you to assume that they have become 'entrapped' if the muscle is entrapped, then it cannot allow the eye to move into whatever position it would be in when the muscle is at its lengthened position. So in this case, It is the inferior rectus being entrapped in a functionally shortened position that is preventing upward gaze.
submitted by soph(45), 2019-07-27T01:49:30Z
its bc this are the only 2 muscles on the orbital floor google orbital floor muscles in google imageshttps://www.google.com/search?q=orbital+muscles&tbm=isch#imgrc=NNOONaLRFuEP1M:
submitted by burak(37), 2019-08-07T20:26:07Z
Orbital floor fracture:
1- Infraorbital nerve injury: Numbness and paresthesia of the upper cheek, upper lip, upper gingiva.
2- Entrapment of the inferior rectus muscle: Impaired upward gaze
3- Enophtalmosis
4- Clousing of maxillary sinus: Teardrop sign
submitted by sympathetikey(816), 2019-06-12T22:43:34Z
.jpg "Medial rectus definition")
Inferior oblique = helps you look up & in.
Also, they said floor of the orbit, so it makes sense that the inferior muscles would damaged.

submitted by niboonsh(241), 2019-06-24T02:08:49Z
The obliques do the opposite action of their name. Inferior oblique moves the eye UP and OUT (extortion, elevation, ABduction). Since the question says that there is a fracture involving the orbital floor, that automatically rules out D (medial rectus and inferior oblique), leaving the only logical answer to be the inferior rectus and inferior oblique. https://www.youtube.com/watch?v=lWKkHWWDIEI
The extraocular muscles are classified into 2 groups: voluntary and involuntary.
Voluntary Muscles
There are 7 voluntary muscles in the orbit. Of those, 6 muscles move the eyeball and 1 muscle moves the upper eyelid.
The muscles moving the eyeball are 4 recti and 2 oblique muscles. The 1 which moves the upper eyelid is named levator palpebrae superioris:
- 4 recti muscles.
- Superior rectus.
- Inferior rectus.
- Medial rectus,
- Lateral rectus.
- 2 oblique muscles.
- Superior oblique,
- Inferior oblique.
- 1 levator palpebrae superioris.
Involuntary Muscles
There are only three automatic/ smooth muscles, viz. superior tarsal or Muller’s muscle, inferior tarsal and orbitalis.
Recti Muscles
Origin: All the recti originate from the corresponding margins of the common tendinous ring. The lateral rectus originates by 2 heads.
The common tendinous ring encloses the optic canal and middle part of the superior orbital fissure. It’s connected medially to apex of the orbit and laterally to a small tubercle (tubercle of Zinn) on the lower border of superior orbital fissure.
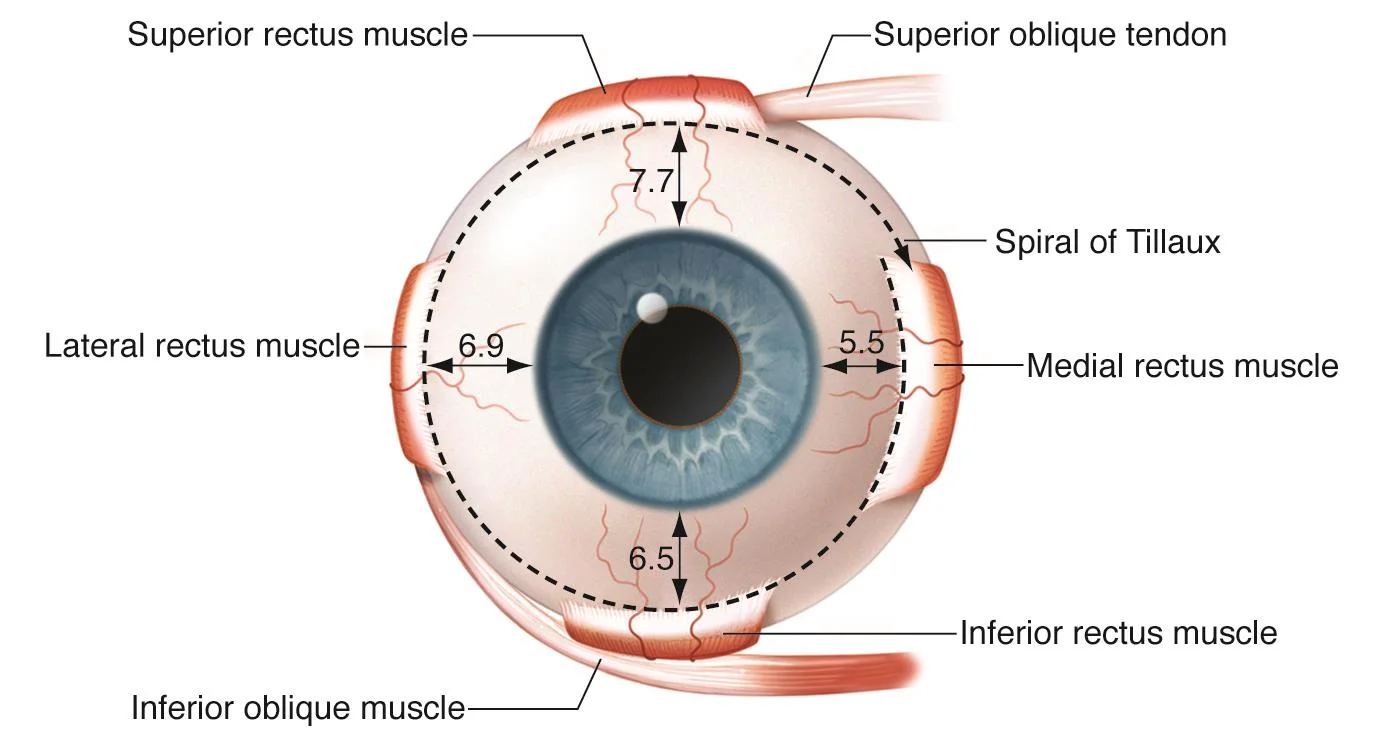
Insertion: All the recti are added into sclera little posterior to the limbus (corneoscleral junction) in front of the equator of the eyeball. Typical space from limbus is: Medial rectus, 5 millimeters Inferior rectus, 6 millimeters Lateral rectus, 7 millimeters Superior rectus, 8 millimeter
Oblique Muscles
The oblique muscles of the orbit are superior and inferior. Their origin and insertion are as follows:
Superior Oblique
Origin: from body of sphenoid superomedial to the optic canal.
Insertion: into sclera supporting the equator in posterior superior quadrant of the eyeball, between the superior rectus and lateral rectus. The tendon of superior oblique goes through a fibrocartilaginous pulley connected to the trochlear notch in the anterolateral part of the roof of the orbit.
Medial Rectus And Inferior Oblique Dmg Muscle
Inferior Oblique
Origin: from rough feeling in the anteromedial angle of the floor of orbit, lateral to the lacrimal groove.
Insertion: into sclera supporting the equator in the posterosuperior quadrant of the eyeball a little below and posterior to the insertion of superior oblique.
Nerve Supply: all the extraocular muscles that move the eyeball are supplied by the oculomotor nerve (CN3) with the exception of lateral rectus and superior oblique that are supplied by the abducent nerve (CN6) and trochlear nerve, respectively [mnemonic: LR6, S04, i.e ” LR (lateral rectus) by 6 CN and SO (superior oblique) by 4 CN] Digimon world re digitize decode english codes.
Activities of Muscles on the Eyeball
Extraocular Muscles: Muscle Activity
Both eyes face forwards and their long axes (visual optic axes) is located in sagittal plane, parallel with every other and with medial walls of the orbits. The lateral walls of orbits slope backwards and medially making a right (90°) angle with every other. The ocular muscles and optic nerve come from the apex of the orbit near the rear of the medial wall and pass forwards and laterally to be connected to the eyeball. The activities of superior and inferior recti are, consequently, not straight, despite their name. The superior and inferior oblique muscles, consequently, have to act in concert with 2 recti to be able to generate direct upward and downward movements of the eyeball.
Axis of Movements of the Eyeball
Elevation and depression: around the transverse axis going through the equator.
Adduction and abduction: around the vertical axis going through the equator. Adobe zii mac reddit.
Rotation (torsion): around the anteroposterior axis stretching from anterior post to posterior pole of the eyeball.
When 12 o’clock position of the cornea rotates medially, it is named intorsion and when it rotates laterally, it termed extorsion.
Activities of Individual Muscles
The activities of individual muscles are easily deduced from Starling’s diagram.

Medial Rectus And Lateral Rectus
Extraocular Muscles: Activities of Muscles
They’re as follows:
- Superior rectus (SR): elevation, adduction and intorsion.
- Inferior rectus (IR): depression, adduction and extorsion.
- Medial rectus (MR): adduction.
- Lateral rectus (LR): abduction.
- Superior oblique (SO): depression, abduction and intorsion.
- Inferior oblique (IO): elevation, abduction and extorsion.
Related Movements of the Eyeball
Conjugate movements: when both the eyes move in exactly the same way with visual axes being parallel.
Disconjugate movements: when the axes of both eyes converge or diverge.
Clinical Significance
Strabismus/squint: Unilateral paralysis of an individual muscle as a result of engagement of the nerves creates strabismus or squint (deviation of eye to the opposite side) and may lead to diplopia (double vision). In diplopia, the light from an object isn’t focused on the indistinguishable regions of both retinae. The actual image falls on the macula of the unaffected eye and fictitious image falls on the peripheral part of retina of the paralyzed eye. The examples are as under:
- Muscle paralyzed Nerve included Effects.
- Lateral rectus Abducent Medial squint.
- Medial rectus Oculomotor Lateral squint.
LevatorpalpebraeSuperioris (Lps) Muscle
Medial Rectus And Inferior Oblique Dmg Pain
Origin
From undersurface of the lesser wing of sphenoid in the apex of the orbit, above the common tendinous ring by a narrow tendon.
Insertion
The muscle expands as it enters forwards from its origin and splits into 3 lamellae:
- Upper lamella being composed of skeletal muscle enters the orbital septum goes through the fibres of orbicularis oculi to be added into the skin of upper eyelid.
- Intermediate lamella being composed of smooth muscle (superior tarsal muscle) is added on to the upper border of the superior tarsal plate.
- Lower lamella being composed of connective tissue is added on to the superior fornix of the conjunctiva.
Nerve Supply
Striped (skeletal muscle) part is supplied by the upper section of oculomotor nerve.
Unstriped (smooth muscle) part is supplied by the post-ganglionic sympathetic fibres from the superior cervical ganglion.
Activities
Medial Rectus Definition
Elevation of the upper eyelid to open the eye.
Clinical Significance
Paralysis of levator palpebrae superioris: Paralysis of levator palpebrae superioris as a result of participation of the oculomotor nerve results in entire ptosis (drooping of upper eyelid). The lesion of cervical sympathetic chain (as in Horner’s syndrome) leads to partial ptosis (partial drooping of upper eyelid) as it changes only smooth muscle part of LPS.